
Fecal Incontinence Treatment in Phoenix, Arizona
Fecal incontinence, also called bowel incontinence or accidental bowel leakage, is the unintended passage of solid or liquid stool. Some people experience a sudden urge and cannot reach the bathroom in time, while others have leakage without recognizing that it has occurred.
Fecal incontinence can interfere with work, exercise, travel, relationships, and social activities. Although many people feel embarrassed discussing bowel-control problems, fecal incontinence is a medical condition with several available treatment options.
Dr. Aisha Akhtar, a board-certified colon and rectal surgeon in Phoenix, provides confidential evaluation and individualized treatment for fecal incontinence and related anorectal or pelvic-floor conditions.
You do not have to manage bowel leakage alone.
Schedule an appointment with Dr. Aisha Akhtar to identify the cause and discuss appropriate treatment options.
What Are the Symptoms of Fecal Incontinence?
Symptoms vary in frequency and severity and may include:
- Leakage of liquid or solid stool
- Inability to reach the bathroom after a sudden urge
- Stool staining or soiling of underwear
- Leakage without awareness
- Difficulty controlling gas
- Mucus leakage
- Recurrent skin irritation around the anus
- Avoiding activities because of concern about an accident
Some people experience occasional leakage during diarrhea, while others have persistent symptoms related to muscle injury, nerve dysfunction, constipation, rectal prolapse, or another underlying condition.
What Causes Fecal Incontinence?
Normal bowel control depends on coordinated function of the anal sphincter muscles, rectum, pelvic-floor muscles, and nerves. A problem affecting any of these structures can contribute to fecal incontinence.
Common causes include:
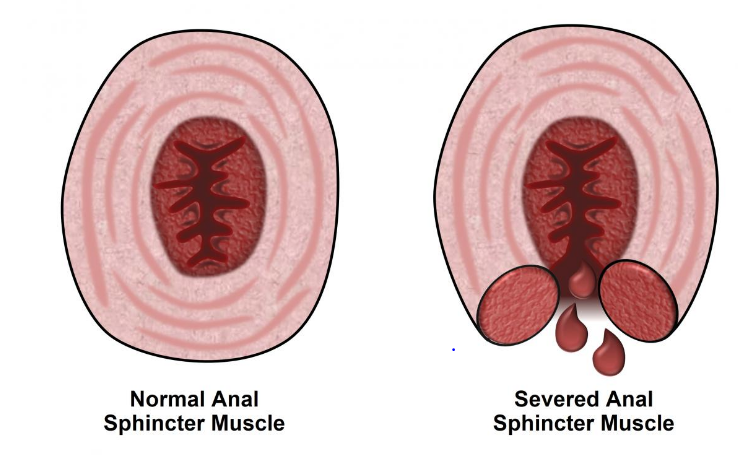
Anal Sphincter Injury
The anal sphincters are circular muscles that help keep the anus closed. They may be weakened or damaged by:
- Vaginal childbirth
- Obstetric tears
- Forceps-assisted delivery
- Previous anal or rectal surgery
- Traumatic injury
Symptoms related to childbirth injuries may appear immediately or develop years later as the muscles weaken with age.
Diarrhea
Loose or watery stool is more difficult to hold than formed stool. Acute infection, irritable bowel syndrome, inflammatory bowel disease, food intolerance, medication effects, or another cause of chronic diarrhea may contribute to leakage.
Constipation and Fecal Impaction
Severe constipation can cause a large amount of hardened stool to become trapped in the rectum. Liquid stool may then leak around the impaction. Chronic straining can also weaken the pelvic floor and affect rectal sensation.
Nerve Damage
Damage to the nerves controlling the anus, rectum, or pelvic floor may occur because of:
- Childbirth
- Diabetes
- Multiple sclerosis
- Spinal cord injury
- Stroke
- Previous pelvic surgery
- Neurologic disease
Rectal Prolapse or Pelvic-Floor Disorders
Rectal prolapse, rectocele, pelvic-floor weakness, and related structural abnormalities can interfere with normal bowel control.
Inflammatory or Structural Disease
Inflammation, scarring, or reduced rectal capacity may result from:
- Crohn’s disease
- Ulcerative colitis
- Previous pelvic radiation
- Rectal surgery
- Tumors or other anorectal conditions
Cognitive or Mobility Impairment
Dementia, limited mobility, or difficulty recognizing the need for a bowel movement may increase the likelihood of accidental leakage.
More than one contributing factor may be present, and occasionally no single cause can be identified.
When Should You See a Colorectal Specialist?
Consider seeking medical evaluation when bowel leakage:
- Happens repeatedly
- Is becoming more frequent
- Interferes with work or daily activities
- Develops after childbirth or anorectal surgery
- Occurs with rectal prolapse
- Is associated with persistent diarrhea or constipation
- Causes significant skin irritation
- Is accompanied by rectal bleeding, pain, unexplained weight loss, or a change in bowel habits
Rectal bleeding should not automatically be attributed to hemorrhoids or fecal incontinence. A medical evaluation may be needed to exclude other colorectal conditions.
How Is Fecal Incontinence Diagnosed?
Evaluation begins with a confidential discussion of your symptoms, medical history, bowel habits, medications, diet, previous procedures, and—in women—pregnancy and childbirth history.
Dr. Akhtar may ask about:
- Whether leakage involves gas, liquid stool, or solid stool
- How often accidents occur
- Whether you feel an urge before leakage
- Diarrhea or constipation
- Previous childbirth injuries
- Prior pelvic, anal, or rectal surgery
- Neurologic or medical conditions
- How symptoms affect daily activities
A physical examination may assess the anus, rectum, pelvic floor, and strength of the anal sphincter muscles.
Diagnostic Tests
Not every patient requires every test. Testing is selected according to the symptoms and suspected cause.
Possible tests include:
Stool studies may be recommended when infection, inflammation, or another cause of diarrhea is suspected.
Endoscopy
Anoscopy, sigmoidoscopy, or colonoscopy may be used to evaluate the anal canal, rectum, or colon when clinically indicated.
Anorectal Manometry
Anorectal manometry measures pressure, sensation, and coordination within the anus and rectum. It may help assess anal sphincter function and guide pelvic-floor therapy or biofeedback.
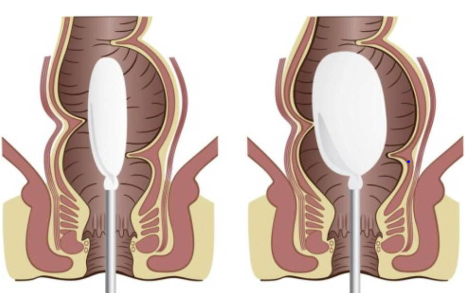
Endoanal Ultrasound
Endoanal ultrasound produces images of the anal sphincter muscles and may identify a muscle defect associated with childbirth, surgery, or trauma.
Pelvic MRI or Defecography
Pelvic imaging may help evaluate the muscles and supporting structures of the pelvis, anus, and rectum. Defecography can also identify rectal prolapse, rectocele, abnormal pelvic-floor movement, or difficulty emptying the rectum.
Additional Testing
Selected patients may require nerve testing, evaluation for chronic diarrhea, or additional gastrointestinal or pelvic-floor testing.
How Is the Severity of Fecal Incontinence Measured?
Symptom questionnaires can help document the type, frequency, and effect of bowel leakage.
The Wexner Fecal Incontinence Score, also called the Cleveland Clinic Incontinence Score, is one commonly used assessment. It considers the frequency of:
- Solid-stool leakage
- Liquid-stool leakage
- Gas leakage
- Use of protective pads
- Lifestyle changes caused by incontinence
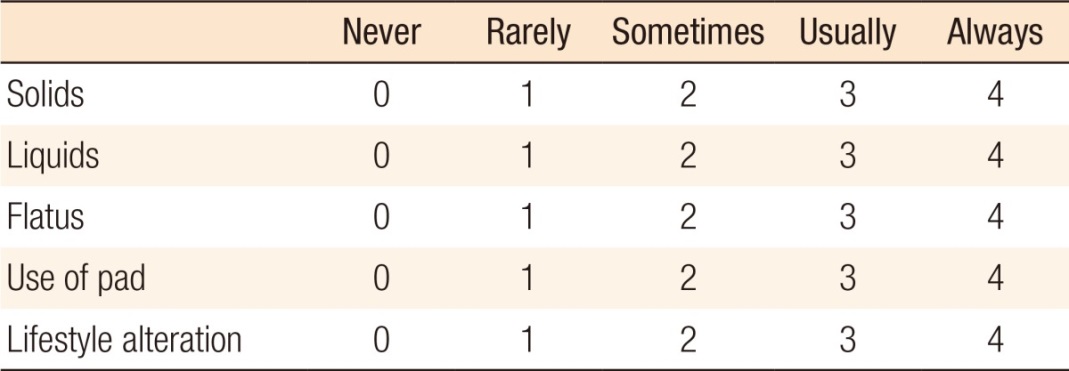
A severity score can help monitor symptoms over time, but treatment decisions should also consider the underlying cause, physical findings, testing results, patient goals, and effect on quality of life.
What Are the Treatment Options for Fecal Incontinence?
Treatment is individualized according to the cause and severity of symptoms. Management commonly begins with conservative measures before progressing to procedural or surgical treatment when appropriate.
Dietary and Bowel-Habit Changes
Improving stool consistency can substantially improve bowel control.
Depending on the underlying problem, recommendations may include:
- Keeping a food and symptom diary
- Gradually increasing dietary fiber
- Drinking an appropriate amount of fluid
- Avoiding foods that consistently trigger diarrhea
- Limiting excessive caffeine or artificial sweeteners when they worsen symptoms
- Establishing a regular toileting schedule
- Treating constipation or fecal impaction
Patients should not make major dietary restrictions without appropriate medical guidance.
Medications
Medication depends on whether the predominant problem is diarrhea, urgency, constipation, or incomplete evacuation.
Options may include:
- Antidiarrheal medication, such as loperamide
- Fiber supplements, such as psyllium or methylcellulose
- Treatment directed at an underlying gastrointestinal condition
- A structured bowel regimen for constipation or overflow leakage
Prescription and over-the-counter medications should be selected according to the cause of symptoms and the patient’s medical history.
Pelvic-Floor Physical Therapy
Pelvic-floor physical therapy can help improve strength, endurance, awareness, and coordination of the muscles involved in bowel control.
Treatment may include exercises designed to:
- Strengthen the pelvic-floor and anal sphincter muscles
- Improve coordination during urgency
- Increase awareness of rectal sensation
- Improve the ability to delay a bowel movement
- Correct abnormal muscle coordination
Kegel Exercises
Kegel exercises involve contracting and relaxing the pelvic-floor muscles. Correct technique is important because repeatedly using the wrong muscles may not improve symptoms.
A pelvic-floor physical therapist can identify the appropriate muscles and develop an individualized exercise program.
Biofeedback Therapy
Biofeedback provides visual or sensory feedback while a patient practices pelvic-floor and sphincter exercises. It may help patients:
- Improve anal muscle strength
- Recognize rectal filling
- Coordinate muscle contractions
- Respond more effectively to bowel urgency
The Emsella Chair is a noninvasive pelvic-floor treatment available for selected patients. It uses electromagnetic stimulation to produce repeated pelvic-floor muscle contractions while the patient remains fully clothed.
Emsella may be considered as part of an individualized treatment plan for pelvic-floor weakness and bowel-control symptoms. It does not replace a colorectal evaluation, and suitability depends on the underlying cause of fecal incontinence, symptom severity, medical history, and examination findings.
Learn more about Emsella Chair treatment in Phoenix, AZ.
Bowel Training
Bowel training involves developing a predictable toileting routine. A clinician may recommend attempting a bowel movement at a consistent time, often after a meal when normal colonic activity is increased.

Sacral Nerve Stimulation
Sacral nerve stimulation, also called sacral neuromodulation, uses a small implanted device to deliver mild electrical impulses to the sacral nerves involved in bowel control.
Treatment generally begins with a temporary trial. Permanent implantation may be considered when the trial produces meaningful improvement.

Sacral neuromodulation may be considered for selected patients whose symptoms have not improved adequately with conservative treatment. Eligibility depends on the cause of incontinence, previous treatments, medical history, and individual goals.
Surgical Treatment
Surgery may be appropriate when fecal incontinence results from a correctable structural problem or when other treatments have not provided adequate control.
Sphincteroplasty
Sphincteroplasty repairs a defined injury in the external anal sphincter, often associated with previous childbirth trauma.
During the procedure, the damaged muscle ends are identified, mobilized, and repaired to restore continuity of the sphincter. Results vary, and function may decline over time. Careful patient selection is therefore important.
Rectal Prolapse Repair
When rectal prolapse contributes to fecal incontinence, correcting the prolapse may improve bowel control. The degree of recovery depends on factors such as symptom duration, sphincter function, nerve function, and the severity of prolapse.
Treatment of Other Anorectal Conditions
Selected patients may benefit from treatment of another condition contributing to leakage, such as significant mucosal prolapse, rectocele, chronic inflammation, or an anorectal structural abnormality.
Hemorrhoid treatment alone does not routinely treat fecal incontinence unless prolapsing tissue or impaired anal closure is contributing to mucus or minor stool leakage.
Colostomy
A colostomy diverts stool through an opening created in the abdominal wall, where it is collected in an external pouch.
This is generally reserved for severe, refractory fecal incontinence when other treatments have failed, are unsuitable, or are not desired. For carefully selected patients, diversion may provide predictable bowel management and improve quality of life.
Why Choose Dr. Aisha Akhtar?
Dr. Aisha Akhtar is a board-certified colon and rectal surgeon who evaluates and treats conditions affecting the colon, rectum, anus, and pelvic floor.
Patients receive:
- Confidential and respectful evaluation
- Assessment by a colorectal specialist
- Treatment directed at the underlying cause
- Conservative, procedural, and surgical options when appropriate
- Individualized recommendations based on symptoms and goals
- Convenient care in Phoenix, Arizona
Frequently Asked Questions
Can fecal incontinence be treated?
Yes. Many patients improve with changes in diet, stool consistency, medication, bowel training, pelvic-floor therapy, or biofeedback. Sacral neuromodulation or surgery may be considered when conservative measures do not provide adequate improvement.
What type of doctor treats fecal incontinence?
A colon and rectal surgeon specializes in conditions affecting the colon, rectum, anus, anal sphincters, and pelvic floor. Gastroenterologists and pelvic-floor physical therapists may also participate in treatment depending on the underlying cause.
Can childbirth cause bowel leakage years later?
Yes. Vaginal childbirth can injure the anal sphincter muscles or their nerves. Some injuries cause immediate symptoms, while others may become apparent years later as the pelvic-floor and sphincter muscles weaken.
Does pelvic-floor therapy help fecal incontinence?
Pelvic-floor therapy can improve muscle strength, awareness, endurance, and coordination. It is most effective when the treatment program is tailored to the patient’s specific muscle function and symptoms.
Is fecal incontinence always caused by a weak sphincter?
No. Bowel leakage may result from diarrhea, constipation, nerve damage, reduced rectal sensation, rectal prolapse, pelvic-floor dysfunction, inflammation, scarring, or several contributing conditions.
Is fecal incontinence the same as diarrhea?
No. Diarrhea refers to loose or watery stool. Fecal incontinence refers to an inability to control stool. Diarrhea can cause or worsen fecal incontinence because loose stool is more difficult to retain.
When is surgery needed for fecal incontinence?
Surgery may be considered when symptoms result from a correctable structural problem, such as an anal sphincter injury or rectal prolapse, or when appropriate nonsurgical treatments have not provided sufficient improvement.
Can rectal prolapse cause fecal incontinence?
Yes. Rectal prolapse can stretch or weaken the anal sphincter, interfere with normal anal closure, and damage the nerves involved in bowel control. Treating the prolapse may improve continence in appropriately selected patients.
Schedule a Confidential Consultation
Fecal incontinence can be physically and emotionally difficult, but effective management options are available. An accurate diagnosis is the first step toward improving bowel control and restoring confidence.
Schedule an appointment with Dr. Akhtar for fecal incontinence evaluation and treatment in Phoenix, Arizona.
Medical content reviewed by Dr. Aisha Akhtar, MD, FACS, board-certified colon and rectal surgeon. This information is educational and does not replace an individualized medical evaluation.








