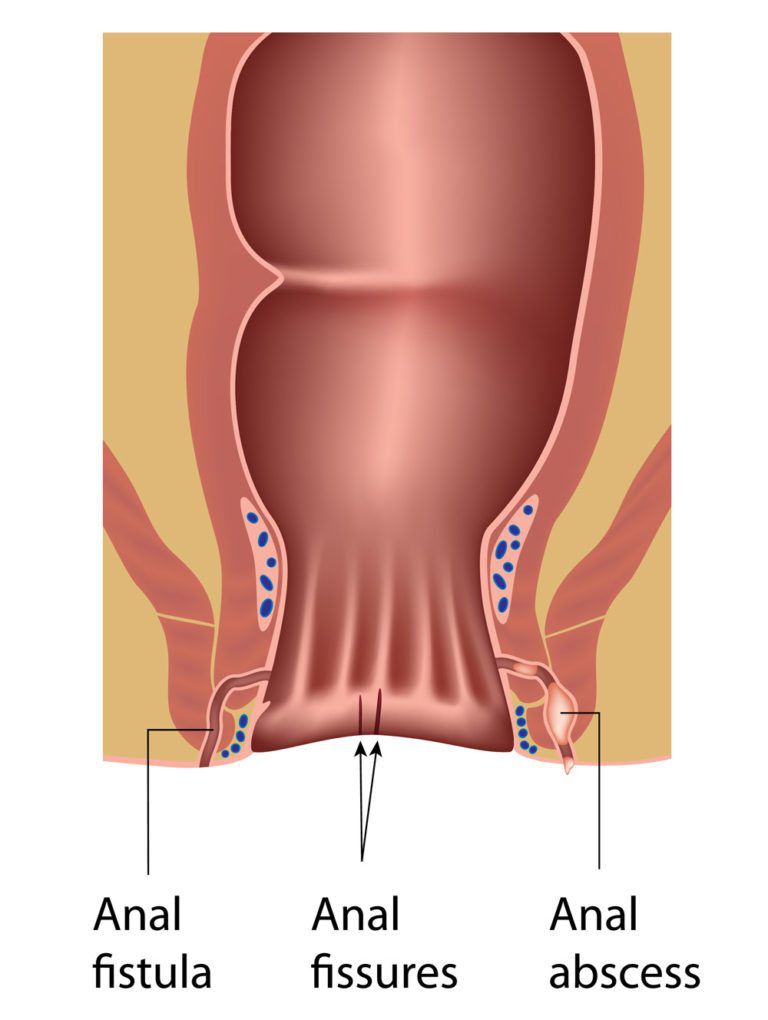
What is Anal abscess and Anal Fistula?
An anal abscess is an infected cavity filled with pus near the anus or
rectum.
An anal fistula is a small tunnel connected outside skin opening to
inside anus opening leading to intermittent discharge outside anus skin.
50% of anal abscesses end up into fistula.
What are the Causes of Anal Abscess and Anal Fistula?
Small glands just inside the anus are part of normal anatomy. If the
glands in the anus become clogged, it may result in an Infection. Local
infection can further lead to formation of abscess. Bacteria, feces, or
foreign matter can also clog the anal glands and cause an abscess to
form. Crohn’s disease, cancer, trauma and radiation can increase the
risk of infections and fistulas.
What are the Symptoms of Anal Abscess and Anal Fistula?
A patient with an abscess may have pain, redness or swelling in the area
around the anal area or canal. Other common signs include feeling ill or
tired, fever and chills. Patients with fistulas have similar symptoms,
as well as drainage from an opening near the anus. A fistula is
suspected if these symptoms tend to keep coming back in the same area
every few weeks.
How Can We Diagnose Anal Abscess and Anal Fistula?
Most anal abscesses or fistulas are diagnosed and managed based on
clinical findings. Occasionally, imaging studies such as ultrasound, CT
scan or MRI can help in the diagnosis and management of deeper abscesses
and may be used to visualize the fistula tunnel.
What are the Treatment Options of Anal Abscess and Anal Fistula?
Anal Abscess:
The treatment of an abscess is surgical drainage under most
circumstances. It is important that your surgeon be very familiar with
treating abscesses and fistula. Colorectal surgeons are experts in this
area. For most patients, an abscess can be drained surgically through a
simple procedure. An incision is made in the skin near the anus to drain
the infection. This can be done at your surgeon’s office with local
anesthetic or in an operating room under general anesthesia. Some
patients with more severe disease may require multiple surgeries to take
care of the problem. Patients who tend to get more severe infections due
to diabetes or immunity problems may need to be hospitalized.

Anal fistula:
Surgery is nearly always needed to treat an anal fistula. They don’t
heal by itself.
There are several different procedures. The best option for you will
depend on the position of your fistula and involvement of control
(Sphincter) muscles.
Sometimes patient needs an initial examination of the area
under anesthesia (where you’re asleep) to help determine the best
treatment option.
The surgeon will talk to you about the options available and which
one they feel is the most suitable for you. Surgery for an anal fistula
is usually carried out under general anesthesia. In many cases, it’s
not necessary to stay in hospital overnight afterwards. The aim of
surgery is to heal the fistula while avoiding damage to the sphincter
muscles (Control muscles), the ring of muscles that open and close the
anus, which could potentially result in loss of bowel control.
Different procedures for fistula are listed below:
FISTULOTOMY:
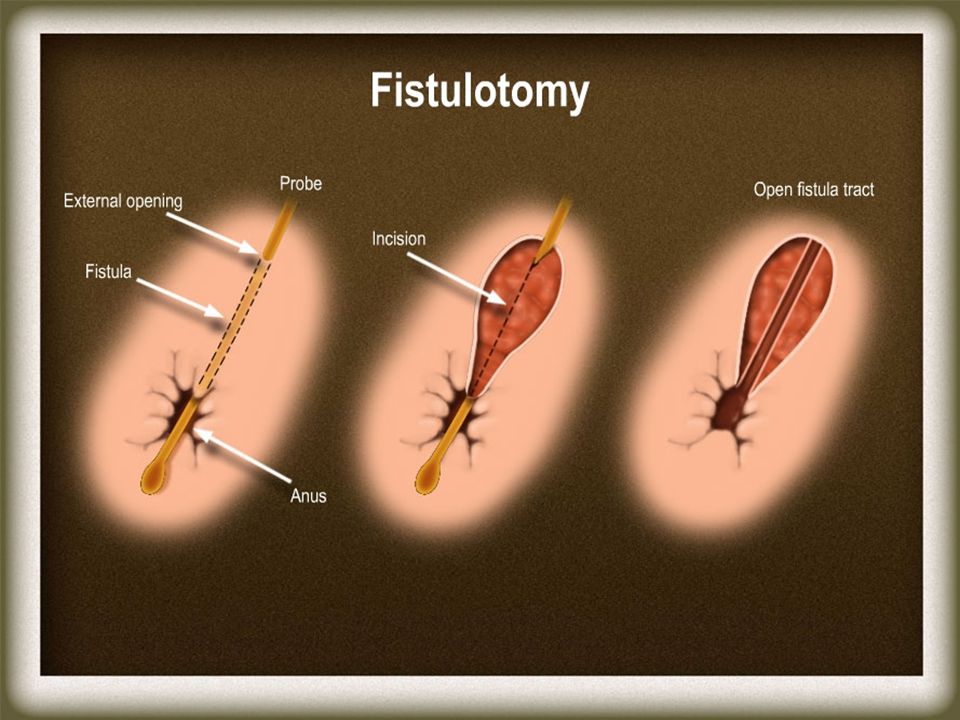
Most common procedure done for fistula. In many patients, if the fistula
is not too deep, a fistulotomy is performed. During this surgery, the
fistula track will be opened to allow healing from the bottom up. The
surgery may require dividing a small portion of the sphincter muscle. A
large amount of the sphincter muscle is not divided as this could lead
to problems with bowel control (fecal incontinence).
If the fistula track does involve a large portion of the sphincter
muscle, other more involved surgeries are done to treat the fistula
without harming the sphincter muscle. More difficult cases may require
multiple surgeries.
Antibiotics alone are not effective in treating abscesses or fistula.
Antibiotics may be needed, in addition to surgery, if a patient has
immunity issues, specific heart valve conditions or widespread
cellulitis (a bacterial infection of the skin and tissues under the
skin). Providing your physician with an accurate medical history and
undergoing a physical exam are important steps in deciding if
antibiotics are required.
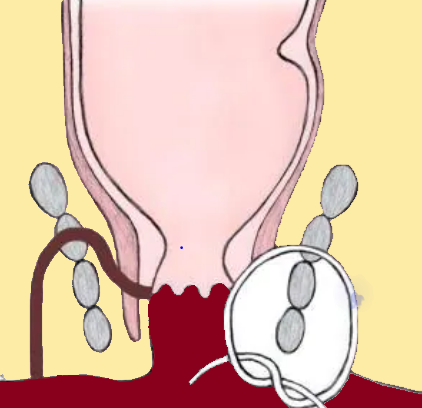
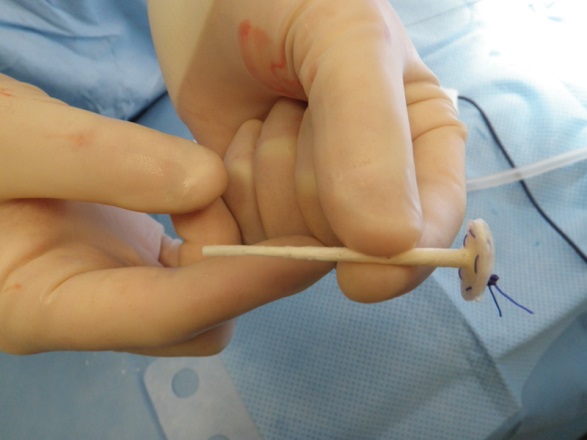
SETON PLACEMENT:
If your fistula passes through a significantly large portion of anal
sphincter muscle or there is local infection, the surgeon may initially
recommend inserting a seton.
A seton is a piece of surgical thread that’s left in the fistula to
keep it open for few weeks. This allows infection to drain and helps
it heal, while avoiding the need to cut the sphincter muscles. Loose
setons allow fistulas to drain and control infection, but do not cure
them. To cure a fistula, other procedure may need. Cutting setons are
not used now a days.
This may require several procedures that the surgeon can discuss with
you.
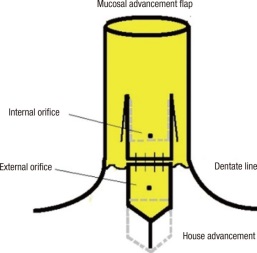
ADVANCEMENT FLAP PROCEDURE:
An endorectal advancement flap procedure may be considered if your
fistula passes through the anal sphincter muscles and carries a high
risk of causing incontinence by performing fistulotomy.
This procedure involves cutting or scraping out the fistula and covering
the hole where it entered the bowel with a flap of healthy tissue taken
from inside the rectum. Outer opening of fistula stays as it is or just
cleans out.
This has a lower success rate than a fistulotomy, but avoids the need to
cut the anal sphincter muscles.
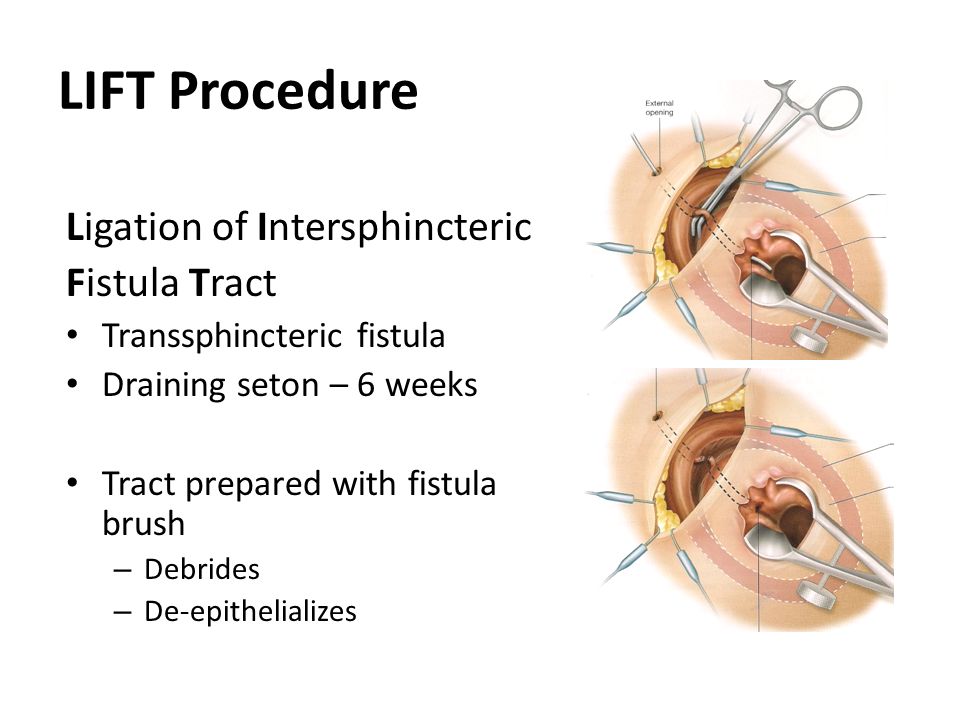
LIFT PROCEDURE:
The ligation of the intersphincteric fistula tract (LIFT) procedure is
also a treatment for fistulas that pass through the anal sphincter
muscles, where a fistulotomy could cause incontinence.
During the treatment, a cut is made in the skin above the fistula and
the sphincter muscles are moved apart. The fistula is then closed at
both ends and cut open so it lies flat. The muscles are not cut.
VIDEOASSISTED ANAL FISTULA SURGERY:
In this procedure, an endoscope (a tube with a camera on the end) is put
in the fistula track. An electrode is then passed through the endoscope
and used to seal the fistula. It is a new procedure and has some
success. It is not widely available and practice.

LASER SURGERY:
Laser treatment involves using a small laser beam to seal the fistula.
There are uncertainties around how well it works.
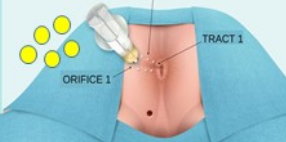
FIBRIN GLUE:
Treatment with fibrin glue is currently the only non-surgical option for
anal fistulas. It involves the surgeon injecting a glue into the fistula
while you’re under a general anaesthetic. The glue helps seal the
fistula and encourages it to heal.
It’s generally less effective than fistulotomy for simple fistulas and
the results may not be long-lasting, but it may be a useful option for
fistulas that pass through the anal sphincter muscles because they do
not need to be cut.
BIOPROSTHETIC PLUG
Another option is the insertion of a bioprosthetic plug.
This is a cone-shaped plug made from animal tissue that’s used to block
the internal opening of the fistula.
This procedure works well for blocking an anal fistula and there are no
serious concerns about its safety.
What Are The Risks Of Anal Fistula Surgery?
Like any type of treatment, treatment for anal fistulas carries a number
of risks.
The main risks are:
infection – this may require a course of antibiotics; severe cases
may need to be treated in hospital
recurrence of the fistula – the fistula can sometimes reoccur
despite surgery
bowel incontinence – this is a potential risk with most types of
anal fistula treatment, although severe incontinence is rare and
every effort will be made to prevent it
The level of risk will depend on things like where your fistula is
located and the specific procedure you have.
POST-TREATMENT PROGNOSIS:
Your surgeon will advise you on proper postsurgical care. Unfortunately,
despite proper treatment and complete healing, an abscess or a fistula
can come back. If an abscess comes back, it suggests that perhaps there
is a fistula that needs to be treated. If a fistula comes back,
additional surgery will likely be required to treat the problem.
Dr. Akhtar will make sure that you know all of your options and choose
the right procedure.








